
This two-part series was possible thanks to a 2016 Reporting Fellowship from the John Jay College of Criminal Justice and the Harry Frank Guggenheim Foundation.
CONCORD, NH – Dr. Anne Johnston, a neonatologist, remembers a time when she had a lot more conflict with child protection workers.
When social services received a report that a pregnant woman was an opioid addict, or that a baby had been born with opioid withdrawal symptoms, a state investigator would come to the hospital and start asking the woman pointed questions. “I would think, ‘Why are you doing this? This mother seems very nice,’” Johnston recalls.
Read Part 2: Child Welfare & Opioid Addiction, Part 1: Striking a Balance of Protection, Treatment
“That’s not a very educated way of looking at things,” she recognizes now. “We often see families at their best, and child protection workers don’t always see that.”
The opioid addiction crisis at times puts the roles of agencies and institutions charged with protecting the health and safety of children at odds and, as a result, collaboration to achieve shared goals is rare. As the New Hampshire Legislature considers a bill that some fear would have unintended consequences, national models, including one as nearby as Vermont, and research suggest more collaborative approaches can improve outcomes for children and families.
 Prenatal exposure to opioids – and immediate safety concerns that lead to newborns being placed in protective custody – is one of the main aspects of parental opioid use that has affected the child welfare system across the country, and to an even greater extent, in New England.
Prenatal exposure to opioids – and immediate safety concerns that lead to newborns being placed in protective custody – is one of the main aspects of parental opioid use that has affected the child welfare system across the country, and to an even greater extent, in New England.
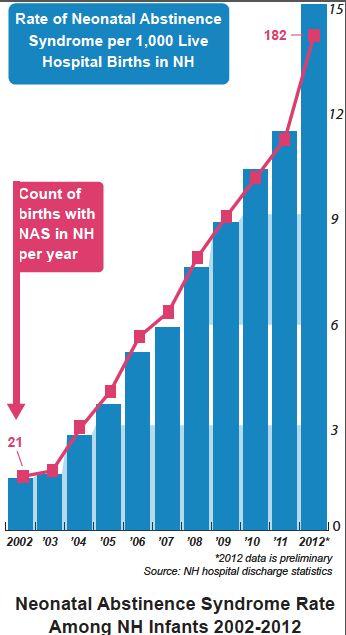
In New Hampshire in 2012, 15 out of every 1,000 babies were diagnosed with neonatal abstinence syndrome (NAS), the clinical terms for the the tremors, sickness and shrill cries that characterize opioid withdrawal in newborns. Although more recent statistics are unavailable, that rate is believed to have increased dramatically in the past few years, as has the rate at which infants and toddlers are entering state protective custody in New Hampshire and nationwide.
Child welfare agencies like the NH Division of Children Youth and Families (DCYF) are mandated to keep children safe. Nationally, over the past few years there has been a shift in the way these agencies view reports of parents who are drug-dependent. In the past, intake workers would press callers for information that would show a child had been harmed; now, harm to the child is generally assumed to have taken place or to be imminent, given the combination of an opioid-addicted caretaker and a very young child. In New Hampshire, the proposed law, Senate Bill 515, would create that presumption in the courtroom as well.
The prevailing view among medical professionals is that the best way to protect babies is to make sure their mothers feel comfortable being straightforward about their drug abuse and can access addiction treatment. From that perspective, reporting all drug-exposed newborns to DCYF would risk the chance that pregnant women would hide their addictions. For DCYF, on the other hand, being informed and working with families to develop safe solutions, and taking children out of potentially dangerous environments, when necessary, is the only way to ensure child safety. “There have been concerns by medical professionals who don’t think they should have to report because the mother is using medications that are legally prescribed,” says DCYF Director Lorraine Bartlett. “It’s inconsistent across the state… You may have medical professionals who don’t think that baby is at risk because the parent is addressing their addiction by taking methadone.”
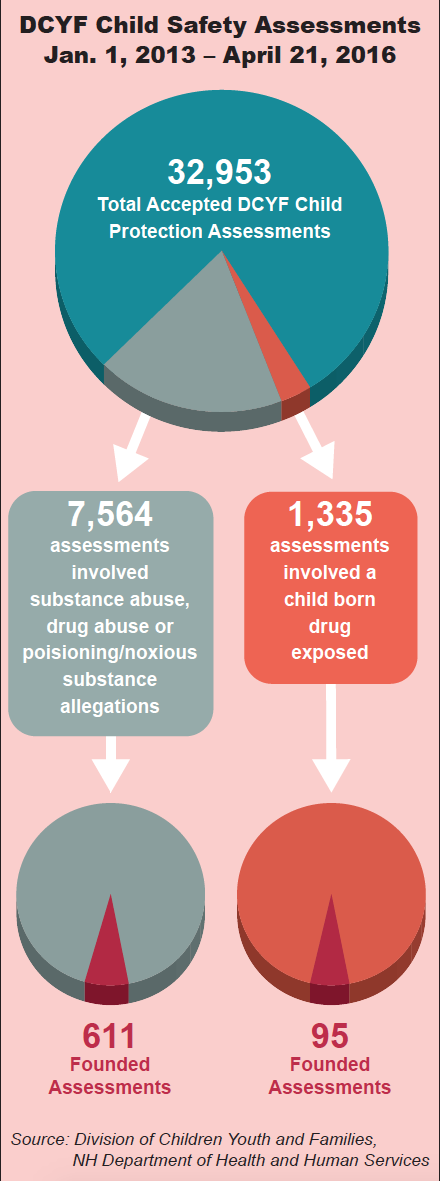
On average, about half of all newborns who have been exposed to opioids in the womb experience withdrawal symptoms that result in a diagnosis of NAS and require medical treatment in the form of gradually decreasing micro-doses of methadone or morphine. Last year, DCYF received 504 reports of children born drug-exposed, up 37 percent over 2014, but Bartlett believes the number of reports is still too low, as some newborns sent home with opioid-dependent parents have not survived.
In 2014 and 2015, there were three infant deaths in New Hampshire of babies two months old or younger in which unsafe sleep – bed-sharing with parents who were using opioids, either illicitly or as prescribed addiction treatment – was suspected as a possible cause, according to a review of records by the NH Medical Examiner’s Office. One of the babies had been diagnosed with NAS. The cause and manner of death in all three cases was undetermined, so it is unknown whether these deaths were preventable. “Babies that have been exposed to opiates are at increased risk statistically to sudden infant death, because of what the opiate exposure has done to the arousal system in the brain,” said Dr. Thomas Andrew, New Hampshire’s chief medical examiner.
These tragic deaths have amplified the tension between child welfare and the healthcare community. That tension has played out in New Hampshire over the past few months, in debates over SB 515, which would make it easier for an already overburdened DCYF to intervene in cases involving parental drug-dependence. Drafted in consultation with DCYF, the bill, as amended, would change current law so that when DCYF files a petition alleging neglect, evidence of a parent’s opioid abuse or dependence would create a presumption that the child’s health has suffered or is very likely to suffer serious impairment. A parent could rebut the presumption with evidence of compliance with treatment for their substance abuse disorder.
⇒ There’s much more to this story. Click here to read it on NH Bar News.